
After an incredibly challenging year responding to the Covid-19 pandemic, care systems are taking stock of lessons learned. Responding to changing population needs has always been a critical aim of person-centred care, especially in light of renewed attention on health inequalities. Our report in October highlighted the racial and gender inequalities in Covid-19 outcomes, finding that death rates are 3.3 times and 2.4 times higher among black men and women respectively than among their white peers. Advancing health equity is best done by listening to people and local communities.
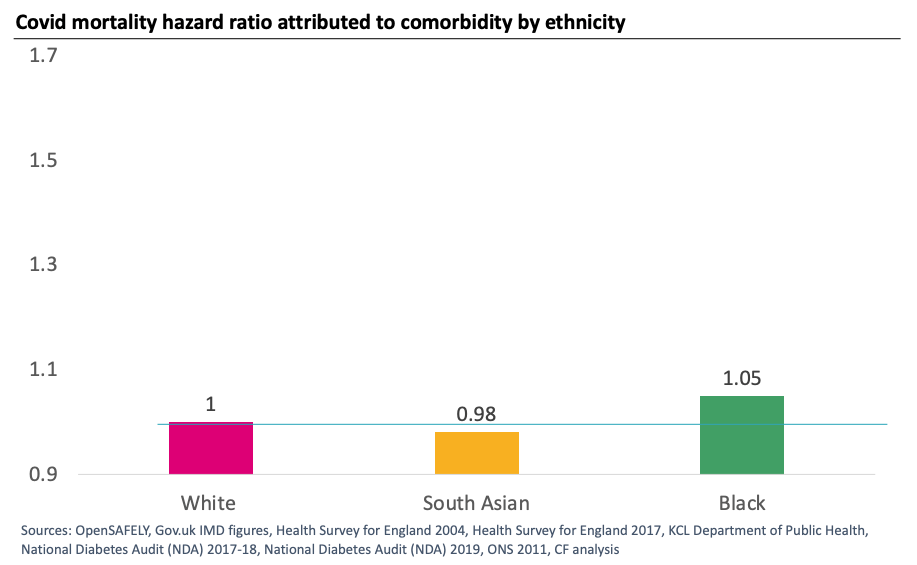
‘Figure 1: Documented co-morbidities do not account for increased risk of death from Covid in Black and Asian people’
As we move forward into a new planning year with big legislative changes, developing systems will need to consider who is best placed to enact change for populations at various geographical levels.
The concept of place is central to the recent DHSC white paper, Integration and Innovation: working together to improve health and social care for all. The white paper describes the purposes of integrated care systems, including “tackling unequal outcomes and access” and notes the “primacy of place” as a delivery vehicle. While places are often aligned to CCG or local authority boundaries, the white paper recognises the heterogeneity of places and the importance of local determination to self-organise in order to best deliver improvements for local populations.
Strong relationships across the NHS, local government, and the third sector are vital to realising the vision for places. The proposed ICS NHS Bodies and Health and Care Partnerships will have statutory duties to regard Health and Wellbeing strategies and Joint Strategic Needs Assessments, but to be successful and turn the dial on health inequalities will require relentless commitment to collaborate at a local level.
Trusted relationships are going to be vital, working across NHS, local government, third sector and wider partners to respond to population needs. Primary Care Networks (PCNs) will also play a critical partner role in places in addition to their role in people’s neighbourhoods.
Plenty of tricky issues remain to be resolved – the dynamics between two tier local authority structures within a place or the potential for boundary changes being just two examples.
To respond to community voices, representative views will need to be heard at all levels of ICS structures, including at place. This won’t be easy to get right but a commitment to achieving it in places is a good first step.
There is a question about the readiness of organisations to work collaboratively at place and take on greater accountability, especially for areas used to traditional system planning and provision roles. Not all places have a history of joint planning and delivery, and ICSs have a role to play to help develop and support places to meet the needs of their local populations.
Empowering places won’t happen overnight as different places need to develop at different speeds. Some areas have long histories of joint working already and know what needs to be done, whereas others are yet to embrace ways of cooperative working.
The ongoing journey to get care right in places won’t be easy but with commitment to the core purpose of improving the lives of residents, much can be achieved.


")
